Every experienced implant clinician has encountered this patient. The bone volume is inadequate for any conventional endosteal placement. Grafting carries risk — or has already been attempted and failed. The options that work for most patients do not apply here. The patient needs full-arch rehabilitation, and the standard implant playbook has run out of pages.
For dental clinics treating severe bone atrophy, this is not a rare or exceptional case. It is an increasingly common clinical reality — and one that demands a treatment approach built specifically for it.
Custom subperiosteal implants exist precisely for this patient population. Designed to rest on the bone surface rather than within it, they eliminate the bone volume requirement that makes endosteal implants impossible in severely atrophic cases. But the clinical outcome of any subperiosteal rehabilitation depends entirely on the quality of the manufacturing behind the implant. Understanding how that manufacturing works — and what it requires — is essential for any dental clinic considering this treatment pathway.
This article explains the full custom manufacturing workflow for subperiosteal implants, from anatomical data intake through surgical delivery, and what dental clinics should look for in a manufacturing partner capable of supporting this level of clinical complexity.
Severe Bone Atrophy and the Limits of Conventional Implant Protocols
Bone loss following tooth extraction is continuous, progressive, and cumulative. For patients who have been edentulous for years — or who have worn full dentures for a decade or more — the residual ridge that remains may bear almost no resemblance to the anatomy the endosteal implant system was designed for.
In the most severe cases, the maxillary ridge resorbs to a thin, fragile shelf. The mandibular symphysis narrows to a dimension that precludes any fixture of meaningful diameter. Sinus pneumatization fills the upper jaw with air where bone should be. Inferior alveolar nerve migration brings the nerve to the very crest of the mandibular ridge, leaving no vertical clearance for an endosteal implant of any length.
For these patients, bone augmentation protocols — sinus lifts, block grafts, distraction osteogenesis — carry significant morbidity, unpredictable regenerative results, and meaningful failure rates, particularly in older patients or those with systemic conditions that compromise bone healing.
The honest clinical assessment is that a meaningful subset of the atrophic patient population cannot be reliably treated with endosteal implants or regenerative preparation. Subperiosteal implant design was developed to address exactly this patient profile.
Why Subperiosteal Implants Are the Clinical Answer for Atrophic Patients
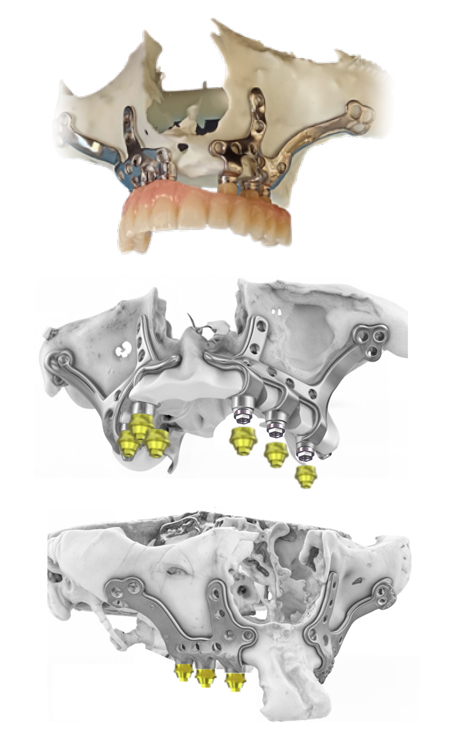
A subperiosteal implant does not require bone volume because it does not enter the bone. Instead, it is positioned on the surface of the bone — beneath the periosteum — where it is held in place by a combination of precise anatomical fit, surgical fixation, and the soft-tissue envelope that heals over the framework.
The prosthetic superstructure is then attached to the abutments that emerge through the mucosa, providing the patient with a fixed, stable, fully functional rehabilitation — without a single endosteal implant in the treatment plan.
This is not a workaround. For the right patient, it is the most biomechanically appropriate treatment option available.
- The Anatomical Case for Surface-Borne Implant Design
In a severely atrophic jaw, the remaining bone surface — even when reduced in height and width — often retains enough area and density to support a well-distributed subperiosteal framework. The key is load distribution: a properly designed framework spreads the prosthetic forces across the maximum available bone surface, preventing the point concentration that would rapidly compromise a conventional implant in diminished bone.
This is why the framework geometry matters so much. A subperiosteal implant designed to genuinely conform to the patient’s bone surface — following every contour, bridging every morphological detail — achieves a distribution profile that a generalized design cannot replicate. Custom manufacturing is not a premium option in these cases. It is the mechanism by which the implant works at all.
- Subperiosteal Implants vs. Bone Grafting and Sinus Lifts in Severely Atrophic Cases
Clinicians evaluating treatment options for severely atrophic patients often face a choice between attempting to create the bone that is missing — through grafting, sinus augmentation, or distraction — and working with the anatomy that exists.
Regenerative approaches are appropriate and highly effective for many patients. But for those with extreme atrophy, a history of prior failed grafts, systemic conditions affecting bone metabolism, or age profiles that compromise healing potential, the risk-benefit calculation changes significantly.
Custom subperiosteal implant design bypasses this calculation entirely. There is no grafting, no bone creation, no waiting for regenerative consolidation. The implant is designed for the patient’s anatomy as it actually is — and the patient’s rehabilitation timeline reflects that directness.
How Custom Subperiosteal Implant Manufacturing Works — The Full Process
The term «custom» should mean something precise in subperiosteal implant manufacturing. At ZPSG, it refers to a full engineering and design process driven entirely by the patient’s individual anatomy — not an adaptation of a standard template, but a framework built from the ground up for one specific patient.
Here is how that process works.
Step 1 — Anatomical Modeling from CBCT Data
Every custom subperiosteal implant begins with the patient’s volumetric imaging data. A high-quality CBCT scan provides the three-dimensional information our engineering team uses to construct an accurate anatomical model of the patient’s jaw.
This modeling process goes beyond rendering a surface. Engineers identify the bone topography in detail — ridge contours, undercuts, concavities, the course of the inferior alveolar nerve, sinus boundaries, and any anatomical features that will influence framework geometry. The result is a precise digital representation of the patient’s bone surface that will guide every subsequent design decision.
This stage sets the ceiling for the manufacturing quality that follows. The more accurately the anatomy is captured and interpreted, the more precisely the implant can be designed to serve it.
Step 2 — Patient-Specific Framework Design and Clinical Collaboration
With the anatomical model established, the framework design phase begins. This is where engineering and clinical knowledge intersect most directly.
Bar geometry, abutment positioning, cross-arch load distribution, fixation screw locations, and emergence profiles are all determined in reference to the specific patient’s anatomy and the prosthetic plan the surgical team has established. Design decisions are not made in isolation — they are made in the context of the full rehabilitation: what the patient needs prosthetically, how the surgical team will approach the placement, and how the restorative laboratory will work with the delivered framework.
At ZPSG, the design is shared with the clinical team before manufacturing begins. This is not a formality. It is a genuine collaborative review in which the surgeon can examine the design, raise anatomical or prosthetic concerns, request modifications, and confirm that the plan is aligned with their clinical intent. Manufacturing only proceeds once this approval is in place.
Step 3 — Precision Fabrication and Material Standards
The approved design is then translated into a physical framework using precision digital fabrication processes with medical-grade materials appropriate for long-term intraoral performance. The fabrication parameters are calibrated to reproduce the approved geometry without deviation — maintaining the topographical accuracy established in the design phase throughout the manufacturing process.
The margin for error at this stage is extremely small. A subperiosteal framework that deviates meaningfully from its approved geometry will not achieve passive fit at placement — and a framework that does not achieve passive fit will underperform clinically regardless of how accurate the design was.
Precision fabrication is where the investment in anatomical modeling and careful design is protected and delivered.
Step 4 — Quality Control Before Surgical Delivery
Before any framework leaves ZPSG for a surgical team, it undergoes a structured quality review. This includes fit verification against the reference anatomical model, structural integrity assessment, surface quality inspection, and a design compliance check confirming that the manufactured implant matches the clinically approved specification.
This stage is not procedural box-ticking. It is the last line of defense between a manufacturing process and a clinical outcome. Every case that ships from ZPSG has passed this review — and any case that does not meet the standard is corrected before dispatch.
What Dental Clinics Should Expect from a Subperiosteal Implant Manufacturing Partner
For a dental clinic integrating subperiosteal treatment into its case mix, the choice of manufacturing partner determines much of what is operationally predictable and clinically reliable about that treatment pathway.
A capable subperiosteal implant manufacturing partner should offer:
- Genuine engineering collaboration — not just file reception, but active clinical dialogue during the design phase
- Design transparency — a clear review and approval step before manufacturing begins, with real ability to adjust
- Reliable production timelines — consistent delivery schedules the surgical team can plan around
- Quality documentation — every case supported by the technical documentation the surgical and restorative team needs
- Accessible communication — a team that responds to clinical questions at planning stage, not just after delivery
- Specialist depth — a manufacturing focus narrow enough that the team has encountered and resolved the kinds of anatomical complexity your most difficult cases present
Clinics that treat their manufacturing partner as a commodity supplier — choosing on price or convenience — typically discover the limitations of that approach when a complex case exposes the gap between a generalist and a specialist.
Integrating Custom Subperiosteal Treatment into a Dental Clinic’s Case Mix
Adding subperiosteal implant treatment for severely atrophic patients does not require a fundamental operational restructuring. With the right manufacturing partner, the process integrates cleanly into the clinical workflow that surgical teams already use.
Patient selection uses existing CBCT capabilities already present in most advanced implant practices. The scan submission process requires a structured data transfer and clinical brief — manageable for any clinic with experience in digital implant workflows. Treatment timelines are predictable once the scan-to-delivery cycle is understood.
What changes is the range of patients a clinic can offer a viable treatment pathway to — and the professional credibility that comes with managing cases that most generalist implant practices cannot.
Global Manufacturing, Local Clinical Impact
ZPSG produces custom subperiosteal implant frameworks for dental clinics and surgical centers across the United States and internationally. The production workflow is designed to support remote clinical teams efficiently — with digital case submission, structured communication protocols, and delivery logistics calibrated for international professional use.
For regional distributors and professional networks seeking to bring this level of custom subperiosteal manufacturing capability to their markets, we also support structured distribution partnerships. You can learn more about how our distributor collaboration model works and what we offer professional partners in each region.
Whether you are a US-based clinic submitting your first complex atrophy case or an international distributor building a specialized implant portfolio, the quality standard is the same.
Manufacturing Quality Is Clinical Quality
In custom subperiosteal implant production, there is no meaningful separation between manufacturing precision and clinical outcome. The accuracy of the anatomical model, the integrity of the design process, the precision of the fabrication, and the rigor of the quality review — these are not operational details. They are the clinical treatment.
A patient with severe bone atrophy who receives a precisely engineered, well-fitted subperiosteal framework experiences a rehabilitation that would otherwise have been unavailable to them. The manufacturing process that produced that framework made the outcome possible.
That is why dental clinics treating the most complex atrophic cases should work with a subperiosteal implant provider whose manufacturing capability is equal to the clinical challenge.
If you have a severe atrophy case to discuss, or you want to understand what integrating custom subperiosteal treatment would look like for your clinic, contact our team. We are ready to work with your anatomy.
FAQs
Q1: Are subperiosteal implants a reliable treatment option for patients with severe bone atrophy?
Yes — when properly designed and manufactured to precise anatomical standards, custom subperiosteal implants offer a clinically validated rehabilitation pathway for patients with severe maxillary or mandibular atrophy who are not candidates for conventional endosteal placement. The reliability of the outcome is closely linked to the quality of the manufacturing process behind the implant.
Q2: What is the difference between a custom-manufactured and a standard subperiosteal implant?
A custom subperiosteal implant is engineered from the patient’s own CBCT scan data to precisely match their bone surface geometry. A standard or adapted design approximates the anatomy using a general template. In severe atrophy, where bone geometry is irregular and highly individual, the precision of custom manufacturing is essential for achieving passive fit — the primary predictor of long-term implant stability.
Q3: How long does the custom subperiosteal implant manufacturing process take from scan to delivery?
The timeline varies depending on case complexity and the manufacturing partner’s workflow. The process typically includes scan intake and anatomical modeling, a collaborative design and approval phase with the clinical team, fabrication, and quality review before dispatch. Clinics working with a specialized, organized manufacturer like ZPSG can plan around a reliable and consistent production schedule communicated at the time of case submission.
Q4: What clinical data does a dental clinic need to submit for custom subperiosteal implant manufacturing?
The minimum requirement is a high-quality CBCT scan of the patient’s relevant jaw anatomy, along with a clinical brief covering prosthetic goals, bone status notes, and any relevant surgical history. The manufacturing partner’s engineering team will typically request additional information if needed during the design review phase.
Q5: Can subperiosteal implants be used in both the maxilla and mandible for severe atrophy cases?
Yes. Custom subperiosteal implant frameworks can be designed for both the maxilla and the mandible, with geometry adapted to the specific anatomical characteristics and bone surface availability of each case. Severe maxillary atrophy with extensive sinus pneumatization and severely resorbed mandibular ridges are both within the design scope of patient-specific subperiosteal manufacturing.
